
Foot and ankle fractures range from simple stress cracks to complex, joint-involving breaks — and the right treatment depends entirely on the type, location, and stability of the injury. Stable fractures often heal well in a boot or cast within 6–8 weeks, while displaced, unstable, or poor-healing fractures (like Jones, navicular, or Lisfranc injuries) usually need surgical fixation with plates and screws to restore alignment and prevent long-term arthritis. Recovery can take anywhere from 4 weeks to 12 months depending on the fracture, and structured rehab is non-negotiable for getting full function back. If pain, swelling or weight-bearing problems aren't improving — or you're unsure whether surgery is the right call — a specialist review is worth getting early.
Foot and ankle fractures are some of the most common injuries I see in clinical practice.
They can affect anyone, from highly active individuals and athletes to those who have simply had a misstep or fall.
While some fractures are straightforward and heal reliably with non-surgical treatment, others are more complex and require careful assessment and, in some cases, surgery to restore alignment, stability, and long-term function.
In this article, I will guide you through the most common types of foot and ankle fractures, how they are diagnosed, when surgery is necessary, and what to expect in terms of healing and recovery.
To understand these injuries, it is helpful to appreciate the complexity of the foot and ankle.
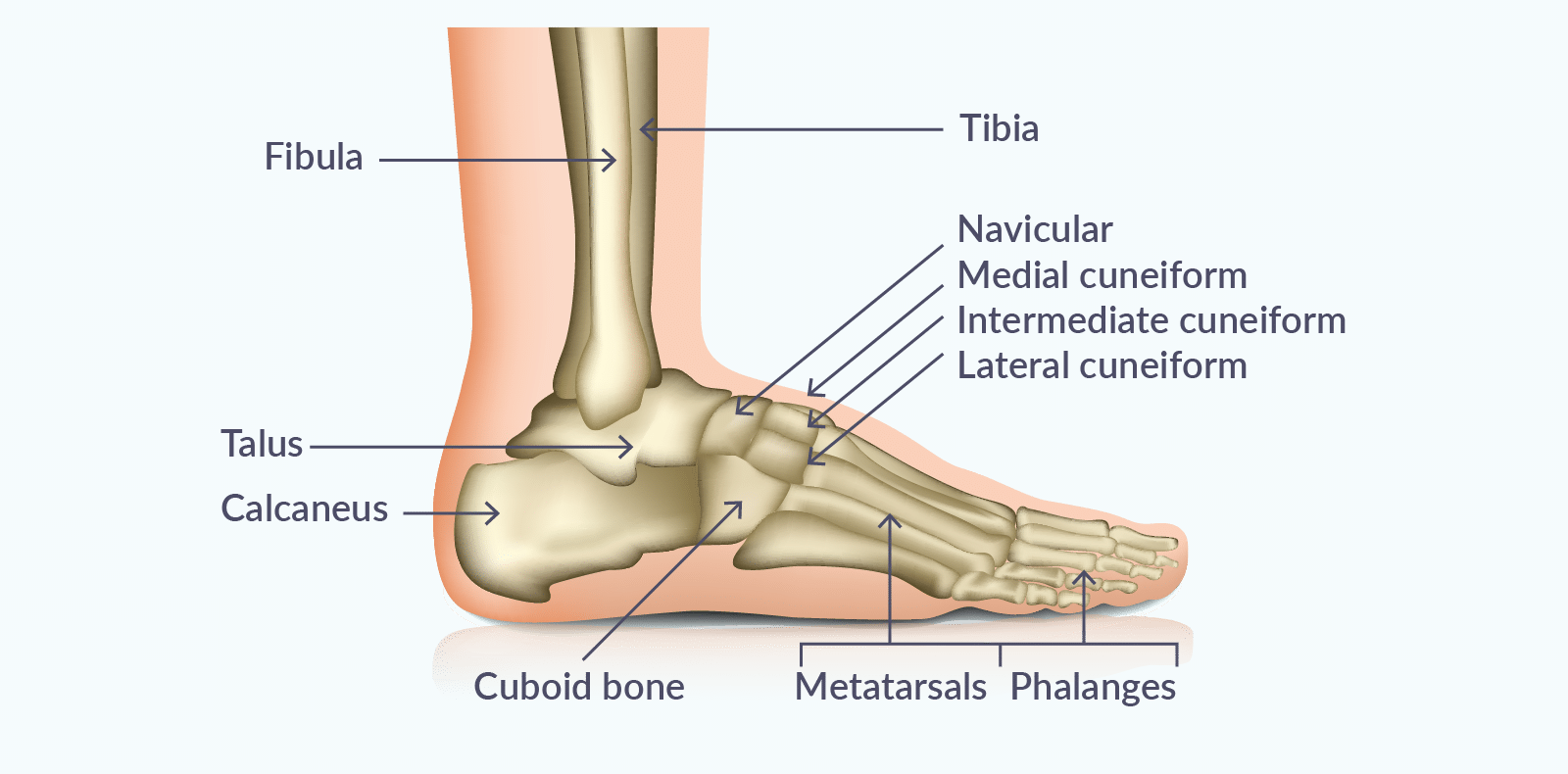
The ankle joint is formed by three bones:
Below this, the foot is made up of 26 bones, divided into:
These structures work together to provide both stability and mobility. When injury occurs, the pattern of the fracture often reflects the forces applied to these bones.

A fracture is a break in a bone, which may be:
Patients will often describe:
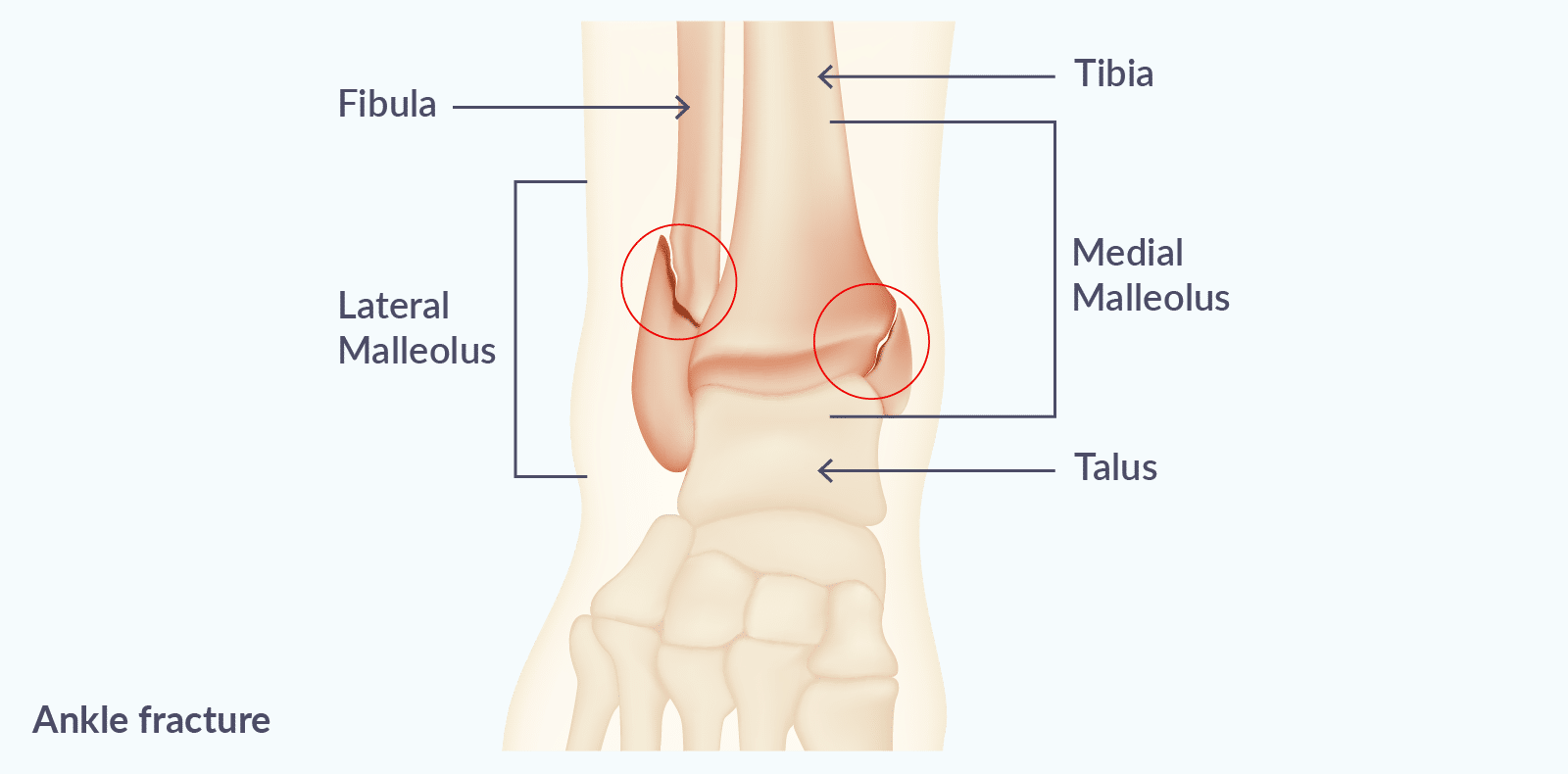
Ankle fractures are among the most frequent injuries I treat and are commonly caused by a twisting mechanism, such as:
The most common patterns include:
A key part of my assessment is determining whether the fracture is stable or unstable, as this directly influences treatment.
Fractures of the fifth metatarsal are particularly common and usually occur with an inversion injury - when the foot rolls inwards.
I commonly see:
Stress fractures are different in that they develop gradually rather than from a single injury.
They are often seen in:
These fractures frequently affect the metatarsals or navicular and can be easy to miss without appropriate imaging.
Calcaneal fractures are typically the result of high-energy injuries, such as:
These injuries can be complex, particularly when they involve the joint surface, and often require specialist surgical input.
Lisfranc injuries affect the midfoot and can involve both fractures and ligament damage.
They are usually caused by:
These injuries are sometimes subtle but can have significant long-term consequences if not identified and treated appropriately.
A thorough clinical examination is essential.
I always assess:
Imaging plays a crucial role in confirming the diagnosis and guiding treatment:
In some cases, particularly with stress fractures or midfoot injuries, further imaging is required even if initial X-rays appear normal.
I am fortunate enough to have access to a full spectrum of imaging so my patients can often have their scan before they see me in clinic.
One of the most important decisions is whether a fracture should be treated surgically or non-surgically.
If a fracture is displaced, meaning the bones are no longer in their correct position, surgery is often required to restore alignment and function.
Fractures involving joints, particularly the ankle, must heal in an optimal position to reduce the risk of long-term arthritis.
Some fractures are more prone to delayed healing or non-union, including:
In active patients, I often recommend surgery in these cases to improve healing and allow a more predictable recovery.
Treatment decisions are always individualised and take into account:
When surgery is required, this usually involves open reduction and internal fixation (ORIF).
This means:
The aim is to restore normal anatomy, allow earlier movement, and reduce the risk of complications such as stiffness or arthritis.
Recovery varies depending on the type of fracture and treatment approach, and also the age and health of the individual.
Rehabilitation is a critical part of recovery. I work closely with physiotherapists to ensure patients follow a structured programme that includes:
This is essential not only for recovery but also for preventing future injury – rehab is a non-negotiable part of the process.
I would always recommend seeking specialist foot and ankle assessment if you experience:
Early diagnosis and appropriate management can make a significant difference to your outcome.
Foot and ankle fractures vary widely, and the correct treatment depends on careful assessment and experience.
My aim is always to provide a tailored approach, whether that involves non-surgical care or operative treatment, to ensure the best possible recovery and long-term function.
As someone with dual training in Foot and Ankle Surgery and Sports & Exercise Medicine, I am able to assess not only the fracture itself, but also the wider factors that influence recovery, including biomechanics, training load, rehabilitation, and return-to-sport goals.
If you are concerned about a foot or ankle injury not progressing as expected, a specialist review can help clarify the diagnosis and guide the most appropriate treatment plan.
Or if you have already been diagnosed with a foot or ankle fracture and would like reassurance about the best treatment approach, a second opinion can often be extremely valuable.
This is particularly true for sports-related injuries, suspected stress fractures, delayed healing fractures, or cases where surgery has been recommended.
No, many foot and ankle fractures heal very well without surgery. Stable fractures, where the bones remain in a good position, can often be treated with a walking boot, cast, or activity modification. Surgery is usually considered when the fracture is displaced, unstable, involves a joint surface, or is unlikely to heal reliably without fixation.
In many cases, yes. Bones have an excellent natural healing ability when they are well aligned and appropriately protected during recovery. The decision depends on the location of the fracture, the degree of displacement, your activity level, and the blood supply to the injured bone.
Certain fractures, such as some fifth metatarsal or navicular injuries, may carry a higher risk of delayed healing and sometimes require surgical treatment.
Most uncomplicated fractures begin to unite within 6 to 8 weeks, but full recovery often takes longer. Swelling, stiffness, weakness, and reduced confidence can persist for several months. More complex fractures, joint injuries, or stress fractures may take 3 to 6 months or longer to fully recover.
The best treatment depends on several factors, including fracture position, stability, involvement of the joint, your general health, and your goals. For example, an athlete or highly active patient may choose surgery to achieve a more predictable recovery in some cases.
A specialist assessment, imaging review, and discussion of your priorities are the best way to determine the right approach.
If a fracture heals in a poor position or fails to unite fully, it can lead to ongoing pain, stiffness, weakness, altered walking pattern, or early arthritis.
If symptoms are not improving as expected, further assessment is required, and we will be able to guide you on the best way forwards.
I would recommend specialist review if you have persistent pain, ongoing swelling, difficulty weight-bearing, delayed recovery, uncertainty about whether surgery is needed, or if you have been told the fracture may be slow to heal.
Early expert input can help avoid prolonged problems and clarify the most effective treatment plan.
Martin Klinke is one of the leading ankle surgeons in London. With an impressive background in both Orthopaedics and Sports Medicine, he takes a comprehensive and compassionate approach to your treatment. He’s a trusted, reputable surgeon who can help get you back in the game!
Mr Martin Klinke offers outpatient consultations at the Cleveland Hospital and the Cleveland Clinic in London.
You can find all his patient reviews here.