Today, I'd like to discuss a common condition known as hammer toe. We'll explore its causes and treatment options and answer some frequently asked questions to provide you with a thorough understanding of this condition.
What is Hammer Toe?
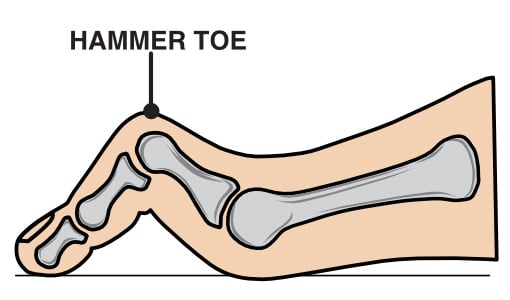
Hammer toe is a deformity that causes one or more of your toe joints to bend upward instead of lying flat.
Hammer toe affects the second, third, or fourth toe results from an imbalance in the muscles, tendons, and ligaments responsible for maintaining toe alignment. If left untreated, the affected toe may progress from being flexible to rigid, leading to increased pain and difficulty walking.
Anatomy of the Toes
The forefoot consists of five toes, each playing a crucial role in balance and movement.
Structurally, four of these toes have three joints: the metatarsophalangeal (MTP) joint at the base, the proximal interphalangeal (PIP) joint in the middle, and the distal interphalangeal (DIP) joint near the tip. However, the first toe, commonly known as the big toe, differs from the others as it has only two joints, the MTP and the interphalangeal (IP) joint.
In cases of hammer toe, the deformity primarily affects the PIP joint, causing it to bend abnormally while the other joints may remain straight or become misaligned over time.
What Is the Main Cause of Hammer Toes?
This condition often results from wearing ill-fitting shoes that force the toes into a bent position over extended periods.
As mentioned, hammer toe is the result of a soft tissue imbalance that puts pressure on the toe muscles, tendons and joints.
High heels or shoes that are too tight can force the foot down and push the toes against the shoe, increasing the pressure and the bend in the toe. If the toe is bent into one position of long enough, the muscles and joints begin to tighten and cannot be stretched out.
Additionally, certain medical conditions like rheumatoid arthritis or diabetes can increase the risk of developing hammer toes due to joint damage or nerve issues.
What are the Symptoms of Hammer Toe?
Hammer toe presents with several noticeable symptoms that can worsen over time.
Initially, you may experience mild discomfort and some hard skin developing on the toes, but as the condition progresses, symptoms can include:
- Toe Deformity: A bend in the middle joint of the affected toe, giving it a hammer-like appearance.
- Pain and Discomfort: Increased pain when wearing shoes, particularly tight or high-heeled footwear.
- Corns and Calluses: Friction from footwear can cause thickened skin to develop over the affected joint.
- Swelling and Redness: Irritation and inflammation around the bent joint.
- Limited Movement: In severe cases, the affected toe may become rigid and difficult to move.
Early recognition of these symptoms will help to ensure effective treatment and prevent longer-term complications.
Diagnosis and Imaging Options
A clinical examination is the first step in diagnosing hammer toe. When you come into the clinic, I will assess your foot’s structure, flexibility, pain levels and mobility.
Imaging studies may be necessary for a more detailed evaluation:
- X-rays: Provide a clear view of bone alignment and joint abnormalities.
- Ultrasound: Assesses soft tissue structures, including tendons and ligaments.
- MRI (Magnetic Resonance Imaging): Helps evaluate severe cases where soft tissue damage or underlying conditions, such as arthritis, may contribute to the deformity.
It is very important to get an accurate and early diagnosis so that we can give you the most appropriate treatment for your specific symptoms and goals.
Can You Correct Hammer Toes?
Yes, hammer toes can be corrected. This can be done surgically or using non-surgical interventions depending on the severity.
Your symptoms and the flexibility of the affected toe play a significant role in determining the best and most effective treatment for you.
In the initial stages, mild hammer toe can be treated with non-surgical interventions when the toe is still flexible.
These may include:
- Footwear Modifications: Switching shoes with a spacious toe box reduces pressure on the toes.
- Orthotic Devices: Custom insoles are used to provide better foot alignment.
- Toe Splints or Caps: Using devices to hold the toe in a corrected position.
- Use Protective Padding: Cushions or pads can prevent friction and reduce discomfort.
- Toe Exercises: Performing specific exercises, with a Physiotherapist or Podiatrist's guidance to strengthen and stretch your toe muscles can help alleviate symptoms.
These methods aim to alleviate symptoms and help prevent further progression of the deformity but are unlikely to correct the condition.
Unfortunately, if the toe has already become rigid then surgical intervention might be necessary to correct the deformity and to give you the best outcome in terms of pain relive, improved mobility and quality of life.
Do Hammer Toe Straighteners Really Work?
Hammer toe straighteners, such as splints or toe caps, can provide relief, especially in the condition's early stages. These devices help in:
- Aligning the Toe: Encouraging the toe to return to its natural position.
- Reducing Discomfort: Minimising friction and pressure from footwear.
- Preventing Further Deformity: Slowing the progression of the condition.
It's important to note that while these devices can alleviate symptoms and provide temporary correction, they may not offer a permanent solution, particularly if the toe has become rigid.
How Do Podiatrists Treat Hammer Toes?
Podiatrists employ a range of treatments based on the severity of the hammer toe. Initial approaches often involve:
- Conservative Measures: Recommending footwear changes, orthotic devices, and specific exercises.
- Medication: Prescribing nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce pain and swelling.
Your treatment will depend on an individual assessment and the progression of the deformity.
I work closely with expert podiatrists to provide a holistic and multidisciplinary approach to your treatment and care.
What Are the Surgical Options for Hammer Toes?
Surgical intervention may be necessary for patients with persistent or severe hammer toe.
Each surgical approach aims to relieve pain, improve toe function, and prevent any further complications.
The choice of procedure depends on whether the toe joint remains flexible or has become rigid.
- Tendon Lengthening: If the toe joint is still flexible, lengthening the tendons responsible for the imbalance can help restore normal toe positioning and function. This procedure alleviates tension and allows the toe to straighten without further structural changes.
- Tendon Transfer: Another option for patients with a flexible toe joint is tendon transfer, where tendons from the bottom of the toe are repositioned to the top. This redistribution of tension helps pull the joint into a straighter alignment and prevents future deformity.
- Arthrodesis (Joint Fusion): For patients with a rigid toe joint, tendon lengthening may be combined with arthrodesis. This procedure involves removing a small section of bone from the affected joint to enable full toe extension.
It is then secured with an external K-wire or pin, which holds the bones in place while they fuse together.
Innovative Surgical Treatments for Hammer Toe
Advancements in medical technology have introduced innovative surgical treatments.
Instead of temporarily holding the operated toe in the corrected position with a pin, an internal implant can be used, which does not have to be removed. In certain situations, these implants are very beneficial.
Additionally, minimally invasive surgical techniques have been developed to correct hammer toes with smaller incisions, reducing recovery time and postoperative discomfort.
Is It Worth Getting Hammer Toe Surgery?
Deciding on whether to have surgery depends on several factors:
- Severity of the Deformity: Surgery may be your best option if the hammer toe is rigid and causes significant pain or interferes with daily activities.
- Response to Non-Surgical Treatments: Surgery may be considered if conservative methods haven't relieved your symptoms.
- Overall Health: If you have any underlying health conditions, this may affect the decision to operate.
Surgical correction can offer long-lasting relief, improved toe function and better mobility, but I will always ensure that all the options are discussed, and we will make an informed decision together.
Surgical Patient

Post-operation hammer toe surgery, second toe on the right foot (left side of photo). The mild hammer toe on the other foot is being treated conservatively at present.
Is Hammer Toe Surgery Painful?
Hammer toe surgery is typically performed as a day case, so you are only in the hospital for a few hours and don’t usually stay overnight. The surgery is often performed under local anaesthetic rather than a general anaesthetic, although this will be discussed individually. You will not feel any pain during the procedure.
Postoperative discomfort varies among individuals, but we ensure that you receive the appropriate medication so you do not have pain.
You can weight bear after the operation and do not need crutches, but as hammertoe operations are often associated with after-forefoot operations, you might need to wear a stiff-soled post-op shoe to protect the operated foot.
It’s important that you follow the postoperative care instructions given to you, to ensure a smooth recovery.
How long does it take to recover from hammertoe surgery?
Recovery from hammer toe surgery varies based on the procedure performed. Initial skin healing from the surgery takes approximately 10-14 days.
Here are some guidelines to recovery timeframes:
- First Few Weeks: You are allowed to weight bear but will benefit from using post-op shoes provided by the hospital and reduce the walking and standing to a minimum to give your bones and joints a chance to heal.
- Four to Six Weeks: Most people can resume walking and light activities, though high-impact exercises should still be avoided.
- Three Months and Beyond: Full recovery, including a return to wearing normal (comfortable and well-fitting) footwear and exercise, is typically achieved within this timeframe.
Long-term outcomes are generally positive, and most patients experience significant pain relief and improved toe alignment and mobility.
Conclusion
Hammer toes are a common foot condition that can cause discomfort and affect daily activities. Early recognition and intervention are key to managing symptoms effectively and potentially avoiding surgery.
Whether through lifestyle modifications, non-surgical treatments, or surgical options, I will ensure that you receive a tailored approach to help you restore function and improve your quality of life.

